Robotic Hysterectomy: Complete Guide to Minimally Invasive Uterus Removal
Categories:

By: Ethan Cole

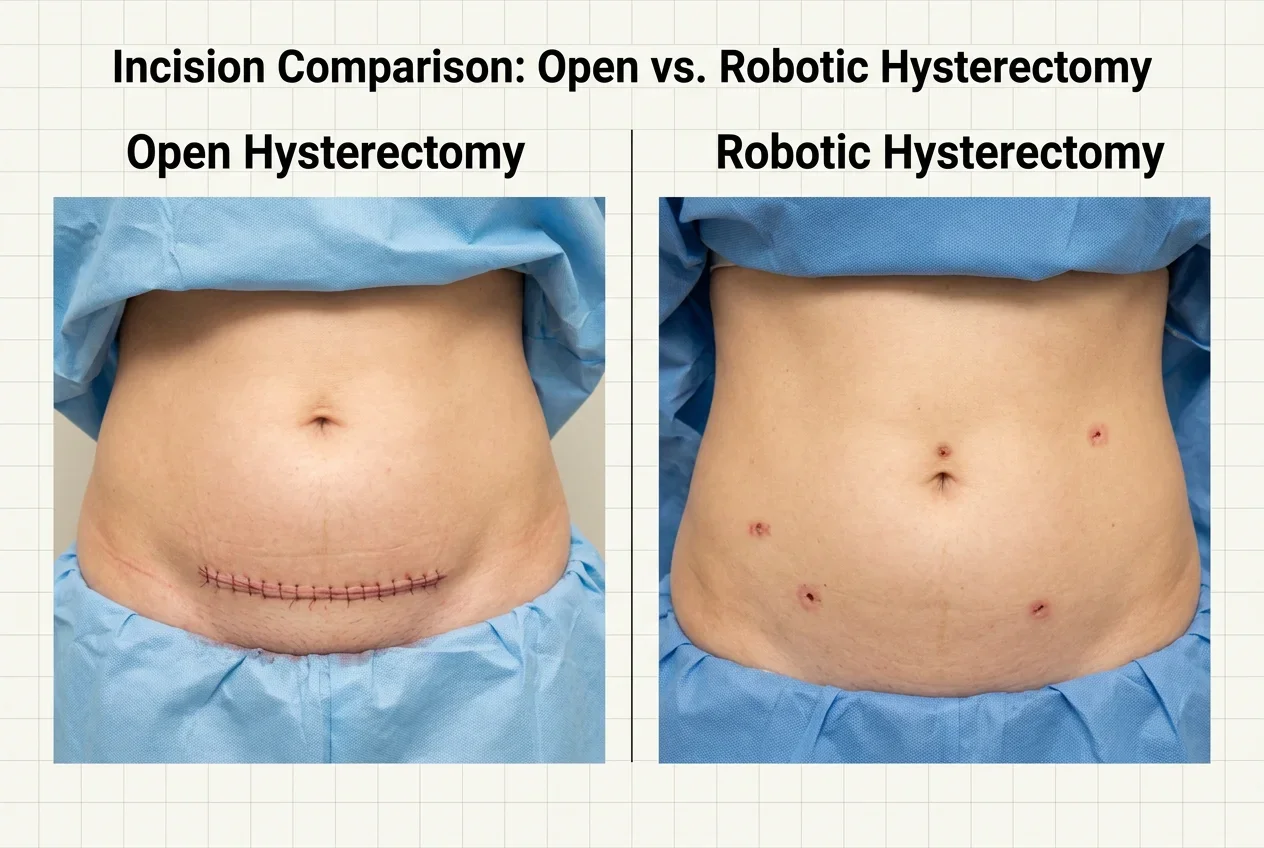
A robotic hysterectomy uses the Da Vinci surgical system to remove the uterus through four to five tiny incisions instead of one large abdominal cut — resulting in less pain, smaller scars, shorter hospital stays, and a recovery measured in weeks rather than months. For women dealing with fibroids, endometriosis, abnormal bleeding, or other conditions that haven't responded to other treatments, this approach offers a modern solution with proven outcomes.
If your gynecologist has recommended a hysterectomy and you're worried about a long, painful recovery, there's a better option. Robotic hysterectomy surgery has transformed how this common procedure is performed — and Dr. Jason Neef, MD, brings this advanced approach to patients right here in the DFW area at Texas Health Huguley Hospital in Burleson.
This guide covers everything: which conditions call for a hysterectomy, the different types of hysterectomy and how they're performed robotically, what your recovery timeline actually looks like, and what life is like after the procedure. No sugarcoating, no vague promises — just the information you need to make a confident decision.
When Is a Robotic Hysterectomy the Right Treatment?
A hysterectomy is typically recommended when gynecologic conditions — heavy bleeding, fibroids, endometriosis, pelvic pain, prolapse, or precancerous changes — haven't responded to medications, hormone therapy, or less invasive procedures. It's not usually the first option your doctor considers, but when conservative treatments fail, it's often the most effective and permanent solution.
Let's be direct about something. No surgeon worth their credentials recommends a hysterectomy as a first-line treatment. You should have already tried other approaches — medications, hormonal IUDs, endometrial ablation, or other conservative options — before this conversation happens. A hysterectomy is a definitive procedure, and it should be treated that way.
That said, there comes a point for many women where the symptoms are severe enough and the conservative options have been exhausted. When that point arrives, a robotic laparoscopic hysterectomy offers the least disruptive way to get permanent relief. Here are the conditions that most commonly lead to this recommendation.
Uterine fibroids are the number one reason women have hysterectomies. These benign growths can cause heavy menstrual bleeding, pelvic pressure, frequent urination, and pain. When fibroids are large, numerous, or keep recurring after myomectomy (fibroid removal), hysterectomy eliminates them permanently. The robotic approach is particularly well-suited for fibroid cases because the enhanced visualization helps the surgeon navigate around large or multiple growths.
Endometriosis causes tissue similar to the uterine lining to grow outside the uterus, leading to chronic pelvic pain, painful periods, and sometimes infertility. When endometriosis is extensive and hasn't responded to medications or excision surgery, hysterectomy — sometimes with removal of the ovaries — can provide definitive relief. Robotic precision helps your surgeon identify and address deep infiltrating endometriosis that might be missed with less advanced visualization.
Abnormal uterine bleeding that doesn't respond to hormonal management or ablation can significantly impact quality of life. Uterine prolapse, where the uterus drops into the vaginal canal, may also require surgical correction. And cervical dysplasia (precancerous cervical changes) that can't be adequately treated with less invasive methods may warrant hysterectomy to prevent progression to cervical cancer.
|
Condition |
Common Symptoms |
Why Hysterectomy May Be Needed |
|
Uterine Fibroids |
Heavy bleeding, pelvic pressure, frequent urination |
Fibroids too large, numerous, or recurrent for conservative treatment |
|
Endometriosis |
Chronic pelvic pain, painful periods, pain during intercourse |
Extensive disease not controlled by medication or excision |
|
Abnormal Bleeding |
Unpredictable heavy periods, bleeding between periods |
Failed response to hormones, IUD, or ablation |
|
Uterine Prolapse |
Pelvic heaviness, bladder issues, tissue protruding |
Moderate to severe prolapse not correctable with pessary |
|
Cervical Dysplasia |
Usually no symptoms (found on Pap smear) |
High-grade changes not treatable by LEEP or cone biopsy |
|
Adenomyosis |
Painful, heavy periods, enlarged uterus |
Condition embedded in uterine wall — no way to remove it without removing uterus |
According to the American College of Obstetricians and Gynecologists (ACOG), a minimally invasive approach should be used whenever technically feasible for hysterectomy. That's exactly what the robotic platform provides — and why Dr. Neef performs the majority of his hysterectomies this way.
What Are the Different Types of Hysterectomy and How Are They Performed Robotically?
There are three main types of hysterectomy — total (removes uterus and cervix), supracervical/partial (removes uterus, keeps cervix), and radical (removes uterus, cervix, and surrounding tissue). The robotic approach can be used for all three, and Dr. Neef determines which type you need based on your specific condition, anatomy, and goals.
The word "hysterectomy" covers a range of procedures, and the type you need depends entirely on why you're having it done. Understanding the differences helps you have a more productive conversation with your surgeon during your consultation.
Total hysterectomy is the most common type. It removes the entire uterus including the cervix. This is the standard approach for most indications — fibroids, abnormal bleeding, endometriosis, and adenomyosis. After a total hysterectomy, you won't need Pap smears for cervical cancer screening unless the procedure was done for a cancerous or precancerous condition.
Supracervical (partial) hysterectomy removes the body of the uterus but leaves the cervix in place. Some women and surgeons prefer this approach because it may preserve more pelvic floor support and potentially reduce certain post-surgical complications. However, because the cervix remains, you'll still need regular Pap smears. This option isn't appropriate for conditions involving the cervix.
Radical hysterectomy removes the uterus, cervix, upper portion of the vagina, and surrounding parametrial tissue. This is typically reserved for certain gynecologic cancers. The robotic approach offers significant advantages for radical hysterectomy because of the extensive dissection required in tight spaces around the bladder, ureters, and blood vessels.
In all three types, removal of the ovaries (oophorectomy) is a separate decision. Ovary removal is sometimes recommended based on your age, cancer risk, and medical history — but it's not automatically included. Dr. Neef discusses this with each patient individually, because removing the ovaries before natural menopause triggers surgical menopause with its own set of implications.
Regardless of which type you need, the robotic approach follows the same basic technique. Dr. Neef works through four to five small port incisions using the Da Vinci system's 3D magnification, wristed instruments, and tremor-filtered precision. The uterus is detached from its supporting structures, the blood supply is secured, and the uterus is removed through one of the small incisions or vaginally. The entire procedure typically takes about one hour.
|
Hysterectomy Type |
What's Removed |
Common Indications |
Still Need Pap Smears? |
|
Total |
Uterus + cervix |
Fibroids, bleeding, endometriosis, adenomyosis |
No (unless done for cancer) |
|
Supracervical (Partial) |
Uterus only, cervix stays |
Fibroids, bleeding (when cervix is healthy) |
Yes — cervix remains |
|
Total + Oophorectomy |
Uterus + cervix + ovaries |
Cancer risk, severe endometriosis, postmenopausal |
No (unless done for cancer) |
|
Radical |
Uterus + cervix + upper vagina + parametrium |
Gynecologic cancers |
Follow oncologist protocol |
Most robotic hysterectomy near me searches lead patients to large medical centers in Dallas or Fort Worth. What many don't realize is that Dr. Neef performs this same procedure right in Burleson — with the added benefit of a community hospital setting, shorter wait times, and personalized attention.
What Does Robotic Hysterectomy Recovery Actually Look Like?
Most women recover from robotic hysterectomy in approximately two to three weeks — dramatically faster than the six to eight week recovery typical of open abdominal hysterectomy. Many patients go home the same day as surgery, manage pain with over-the-counter medication within 48 hours, and return to desk work within two weeks.
Recovery is the single biggest reason patients choose the robotic approach. The difference between going back to your life in two weeks versus being out of commission for two months isn't just a convenience — it's a quality-of-life game changer. Let's break down what you can actually expect, week by week.
Days 1-3: The hardest part. You'll feel sore and fatigued after anesthesia. Some abdominal bloating from the surgical gas is normal and resolves quickly. Most patients use their prescription pain medication for the first two to three days, then switch to ibuprofen or naproxen. Walking short distances around the house is encouraged immediately — it helps with gas discomfort and reduces blood clot risk. You'll need someone to drive you home and help around the house for the first few days.
Days 4-7: Turning the corner. By mid-week one, most patients feel significantly better. You can shower normally, prepare simple meals, and handle basic self-care. The incision sites may feel tender but shouldn't be actively painful. Appetite returns, and energy starts rebuilding. Keep walking — increase your distance gradually each day.
Week 2: Approaching normal. Many women return to desk work or light-duty jobs by the end of week two. You can drive once you're off prescription pain medication and can comfortably look over your shoulder and brake suddenly. Light household tasks are fine. Avoid lifting anything heavier than 15 pounds.
Weeks 3-4: Getting clearance. At your follow-up appointment, Dr. Neef evaluates your healing and typically clears you for more activity. This is when you can gradually resume exercise, heavier housework, and sexual activity. Most women feel fully recovered by week four, though everyone heals at their own pace.
|
Recovery Milestone |
Robotic Hysterectomy |
Open Abdominal Hysterectomy |
|
Hospital Stay |
Same day or 1 night |
2-3 nights |
|
Off Prescription Pain Meds |
2-3 days |
7-14 days |
|
Showering Normally |
Day 2-3 |
After staple/suture removal |
|
Driving |
~1 week |
3-4 weeks |
|
Return to Desk Work |
~2 weeks |
4-6 weeks |
|
Light Exercise |
2-3 weeks (with clearance) |
6-8 weeks |
|
Full Activity |
3-4 weeks |
8-12 weeks |
One thing patients often don't expect: the emotional aspect of recovery. A hysterectomy is major surgery with real emotional weight — even when you're relieved to be done with your symptoms. Some women experience a sense of loss, mood changes, or adjustment to the idea that pregnancy is no longer possible. These feelings are normal and valid. If you had your ovaries removed, surgical menopause may bring hot flashes, mood shifts, and sleep changes that require management. Dr. Neef and his team can help you navigate both the physical and emotional recovery.
Key Takeaways
Robotic hysterectomy removes the uterus through tiny incisions using Da Vinci technology, with most patients going home the same day and recovering in two to three weeks.
Multiple conditions warrant hysterectomy when conservative treatments fail — fibroids, endometriosis, abnormal bleeding, prolapse, adenomyosis, and precancerous changes.
Three main types exist — total, supracervical, and radical — and the robotic approach works for all of them. Ovary removal is a separate, individualized decision.
Recovery is dramatically faster than open surgery: two to three weeks versus six to eight weeks, with most patients managing pain with OTC medication by day three.
Both physical and emotional recovery matter — mood changes, adjustment to body changes, and surgical menopause (if ovaries are removed) are normal parts of the process.
Dr. Neef performs robotic hysterectomies at Texas Health Huguley in Burleson — world-class surgical care without the big-city hospital hassle.
What Changes After a Hysterectomy — and What Stays the Same?

After a hysterectomy, your periods stop permanently and pregnancy is no longer possible. If your ovaries are preserved, you won't experience surgical menopause — your hormones continue functioning normally until natural menopause. Most women report significant improvement in the symptoms that led to surgery, and many wish they'd had the procedure sooner.
The "what happens after" question is one of the most common concerns patients bring to their consultation — and rightfully so. A hysterectomy changes some things permanently, but it leaves many things untouched. Getting clarity on this distinction helps reduce pre-surgery anxiety.
What definitely changes: menstruation stops. You'll never have another period. For women who've been dealing with years of heavy, painful, unpredictable bleeding, this is the entire point — and it's life-changing. You also can't become pregnant after a hysterectomy, which is an important consideration for women of reproductive age.
What often surprises patients: if your ovaries are preserved (and they are in most non-cancer cases), your hormones keep functioning normally. You won't suddenly go into menopause. Your ovaries will continue producing estrogen and progesterone until they naturally decline — usually around the age they would have anyway. This means no hot flashes, no bone density changes, and no HRT needed because of the surgery itself.
If your ovaries are removed, you will enter surgical menopause regardless of your age. This can bring hot flashes, night sweats, vaginal dryness, mood changes, and sleep disruption. Hormone replacement therapy (HRT) is an option many women pursue to manage these symptoms, and Dr. Neef can help you develop an appropriate management plan.
Sexual health after hysterectomy is another common concern. Research consistently shows that most women report the same or better sexual function after hysterectomy — largely because the painful symptoms that were interfering with intimacy are gone. Some women notice changes in sensation, particularly if the cervix was removed, but the vast majority report positive overall outcomes.
Your intestines gradually shift to fill the space where your uterus was — this happens naturally and doesn't cause problems. Pelvic floor exercises (Kegels) and appropriate physical activity support your long-term pelvic health after surgery.
Take the first step toward freedom from gynecologic pain. Schedule your robotic hysterectomy consultation with Dr. Neef — expert care, right here in Burleson.
Call (817) 568-8731Categories:
Frequently Asked Questions
-
Yes — even though it's minimally invasive, a hysterectomy is still major surgery involving removal of an organ. However, the robotic approach significantly reduces the physical impact, with shorter hospital stays, less pain, and faster recovery than open surgery.
-
Most robotic hysterectomies take about one hour. Complex cases involving large fibroids, extensive endometriosis, or additional procedures may take up to three hours.
-
The robotic technique itself doesn't cause weight gain. However, if your ovaries are removed and you enter surgical menopause, hormonal changes can contribute to weight gain. Dietary modification and appropriate exercise help manage this.
-
If you had a total hysterectomy (cervix removed) for a non-cancerous condition, Pap smears are generally no longer needed. If your cervix was preserved (supracervical hysterectomy) or if your surgery was for cancer, regular screening continues.
-
If preserved, your ovaries continue functioning normally — producing hormones until natural menopause. Ovary removal is a separate decision made based on your age, cancer risk, and medical history, discussed individually with Dr. Neef.
-
Hysterectomy significantly reduces endometriosis symptoms, especially if the ovaries are removed (eliminating estrogen production that fuels the disease). In rare cases, endometriosis can recur if ovaries are preserved, but most women experience lasting relief.
-
Most patients can drive within about one week — once they're off prescription pain medication and can comfortably perform emergency maneuvers like braking suddenly and looking over their shoulder.
-
Most women report the same or improved sexual function after hysterectomy, primarily because the painful symptoms interfering with intimacy are resolved. Some women notice changes in sensation, but overall satisfaction is typically positive.
-
Dr. Neef is one of the only surgeons in the DFW area performing robotic laparoscopic hysterectomy surgery on the Da Vinci platform at a community hospital setting. Patients get specialized robotic expertise with the personalized attention and convenience of Texas Health Huguley in Burleson — including valet parking and concierge service.
-
Dr. Neef evaluates every patient individually and explores conservative options first. A hysterectomy is recommended only when other treatments — medications, hormonal therapy, ablation, or less invasive procedures — haven't adequately addressed your condition. Your consultation includes a thorough discussion of all available options.